IMPORTANT SAFETY INFORMATION
CONTRAINDICATIONS
- Oxtellar XR is contraindicated in patients with a known hypersensitivity to oxcarbazepine, or to any of the components of Oxtellar XR, or to eslicarbazepine acetate. Reactions have included anaphylaxis and angioedema.
WARNINGS & PRECAUTIONS
- Clinically significant hyponatremia (sodium <125 mmol/L) may develop during treatment. Measurement and laboratory tests of serum sodium concentrations should be considered for patients during maintenance treatment with Oxtellar XR, particularly if the patient is receiving other medications known to decrease serum sodium levels. Discontinuation of oxcarbazepine treatment may be clinically required.
- Rare cases of anaphylaxis and angioedema involving the larynx, glottis, lips, and eyelids have been reported in patients after taking the first or subsequent doses of oxcarbazepine. Angioedema associated with laryngeal edema can be fatal. If a patient develops any of these reactions after treatment with Oxtellar XR, the drug should be discontinued and an alternative treatment started. Do not rechallenge these patients with Oxtellar XR.
- Approximately 25% to 30% of patients who have had hypersensitivity reactions to carbamazepine will experience hypersensitivity reactions with Oxtellar XR. Patients with a history of hypersensitivity reactions to carbamazepine should ordinarily be treated with Oxtellar XR only if the potential benefit justifies the potential risk. Discontinue Oxtellar XR immediately if signs or symptoms of hypersensitivity develop.
- Serious dermatological reactions, including Stevens-Johnson syndrome and toxic epidermal necrolysis, have been reported in association with oxcarbazepine use. Should a patient develop a skin reaction while using Oxtellar XR, consideration should be given to discontinuing its use. (Please see WARNINGS section of complete prescribing information.)
- Anyone considering prescribing Oxtellar XR must balance the risk of suicidal thoughts or behavior with the risk of untreated illness. Epilepsy and many other illnesses for which antiepileptic drugs are prescribed are themselves associated with morbidity and mortality and an increased risk of suicidal thoughts and behavior. Should suicidal thoughts and behavior emerge during Oxtellar XR treatment, the prescriber needs to consider whether the emergence of these symptoms in any given patient may be related to the illness being treated.
- Withdrawal of Oxtellar XR should be done gradually to minimize the potential of increased seizure frequency and status epilepticus.
- Multi-organ hypersensitivity reactions have occurred in patients on oxcarbazepine therapy. Some of these cases resulted in hospitalization and some were life-threatening. Signs and symptoms of this disorder were diverse; however, patients typically, although not exclusively, presented with fever and rash associated with other organ system involvement disorders. If an alternative etiology cannot be established, discontinue Oxtellar XR.
- Rare reports of hematologic events such as pancytopenia, agranulocytosis, and leukopenia have been seen in patients treated with oxcarbazepine and discontinuation of therapy should be considered if any evidence of these hematologic events develop.
- Due to physiological changes during pregnancy, plasma concentrations of the active metabolite of oxcarbazepine may gradually decrease throughout pregnancy. An increase in seizure frequency may occur. Monitor patients carefully during pregnancy and through the postpartum period.
- Exacerbation of or new onset primary generalized seizures has been reported with immediate-release oxcarbazepine. The risk is seen especially in children, but may also occur in adults. Discontinue Oxtellar XR if it occurs.
- Data on a limited number of pregnancies from pregnancy registries suggest that oral clefts and ventricular septal defects are associated with oxcarbazepine monotherapy use.
DOSING CONSIDERATIONS
- Enzyme inducing antiepileptic drugs such as carbamazepine, phenobarbital, and phenytoin decrease the exposure to MHD, the active metabolite of Oxtellar XR. Dosage increases or discontinuation of enzyme inducers may be necessary.
- In adult patients with severe renal impairment, initiate Oxtellar XR at a lower starting dose and increase, if necessary, at a slower than usual rate until the desired clinical response is achieved.
- Use of Oxtellar XR with certain hormonal contraceptives may decrease hormone plasma levels and render these contraceptives less effective. Additional or alternative non-hormonal forms of contraception are recommended.
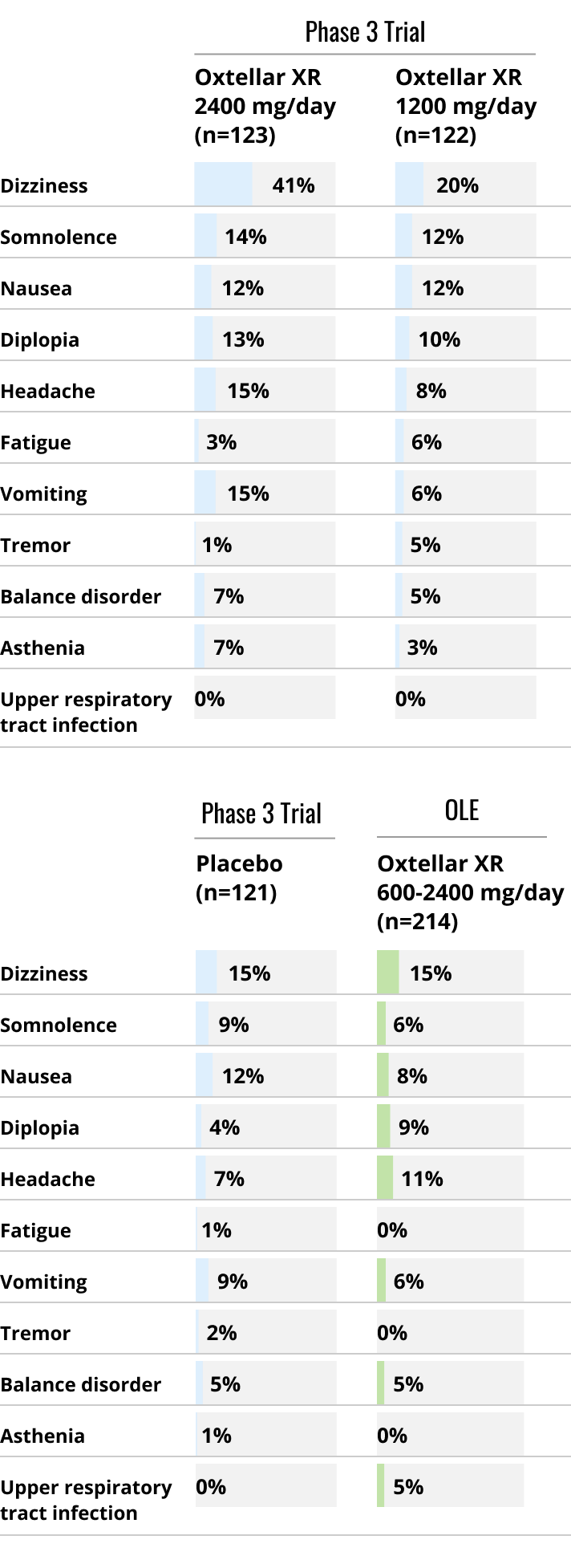
ADVERSE REACTIONS
The most commonly observed adverse reactions (≥ 5% and more frequent than placebo) seen in adults were (1200 mg, 2400 mg, v placebo): dizziness (20%, 41%, v 15%), somnolence (12%, 14%, v 9%), headache (8%, 15%, v 7%), balance disorder (5%, 7%, v 5%), tremor (5%, 1%, v 2%), vomiting (6%, 15%, v 9%), diplopia (10%, 13%, v 4%), asthenia (3%, 7%, v 1%), and fatigue (6%, 3%, v 1%). Adverse reactions in pediatric patients are similar to those seen in adults.
INDICATION
Oxtellar XR is indicated for the treatment of partial-onset seizures in patients 6 years of age and older.
Please refer to the full Prescribing Information and Medication Guide for Oxtellar XR for additional important information.
Oxtellar XR (oxcarbazepine) extended-release tablets for oral use